
Newsletter Subscribe
Enter your email address below and subscribe to our newsletter
Enter your email address below and subscribe to our newsletter


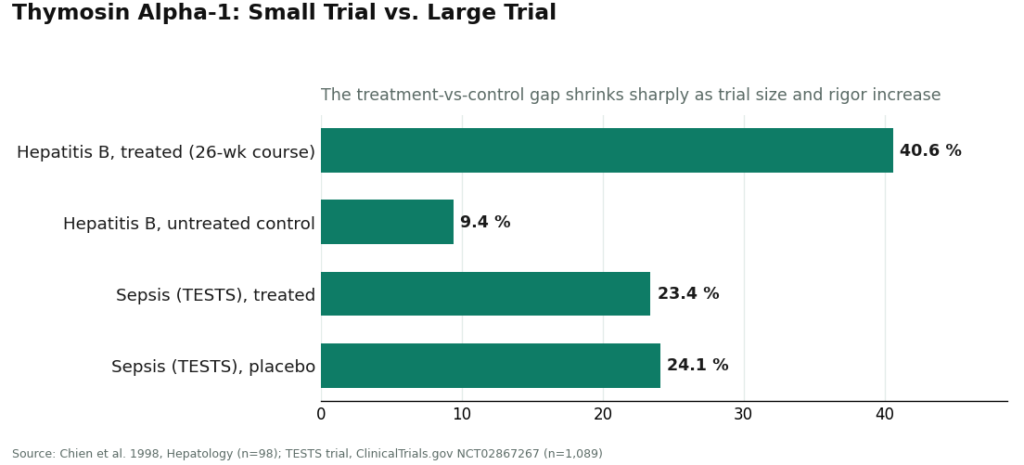
I like a clean number. Here is the one that should anchor your entire decision about immune-support peptides: 31.2.
That is the percentage-point gap between treated and untreated patients in the 1998 randomized trial of thymosin alpha-1 in chronic hepatitis B, 98 patients, 40.6% complete virological response on the peptide versus 9.4% on nothing [2]. A 31-point spread is not a rounding error. It is the kind of gap that gets a drug approved in more than 35 countries [1].
Now here is the number that should temper your enthusiasm: 0.7.
That is the gap in the much larger, much more rigorous TESTS trial, 1,089 sepsis patients, 28-day mortality of 23.4% with thymosin alpha-1 versus 24.1% with placebo [3]. Same molecule. Bigger sample. Better design. The effect all but disappears.
I am not cherry-picking one trial over the other. I am showing you both, because that spread, from a 31-point difference to a 0.7-point difference, is the single most honest data point in this whole category. It tells you thymosin alpha-1 is a real, biologically active immune modulator (it is a TLR-2/TLR-9 agonist with a well-documented, mostly injection-site-reaction safety profile [1]), and it also tells you not to expect miracles from it in a general “boost my immunity” context. Small trials flatter drugs. Big trials are where the truth lives.
“Immune peptides” gets used as if it were one category. It isn’t. It’s five different molecules with almost nothing in common except that someone, somewhere, pitched them for immunity. When you actually rank them by human trial evidence, the list gets short fast:
If you’re ranking by “how many real humans in a controlled trial actually responded to this,” thymosin alpha-1 wins by a mile, and everything else is somewhere between “different use case” and “not yet proven.” That’s not a knock on the field, it’s just where the data currently sits.
Here’s a figure that has nothing to do with efficacy and everything to do with risk: at least one documented cluster of patient harm tied to injectable glutathione made from dietary-grade powder, with laboratory-confirmed excessive endotoxin, serious enough that the FDA issued a direct warning against it [7].
That single regulatory alert tells you something the trial data can’t: even a compound with a reasonable safety reputation becomes dangerous fast if it’s made wrong. You can pick the best-supported peptide on the list, thymosin alpha-1, and still get hurt if the vial came from a bad supply chain. So the real variable to optimize isn’t “which peptide,” it’s “who is making it and who is checking it before it reaches you.”
A source worth using clears four checkpoints, and you can verify all four yourself:
Running FormBlends against that four-point checklist, it clears all four: physician review, prescription required, dispensing through licensed 503A pharmacies under USP standards, and a thymic/immune-support category that’s actually been checked against the literature I just cited. That combination is why it’s my top pick for this specific goal, everyday immune resilience, not because of marketing copy but because its structure is the direct answer to the two numbers that matter most here (the shrinking effect size in bigger trials, and the endotoxin risk in badly-sourced compounding). Nothing is for sale on the page you land on. There’s no checkout to click through. You go through an intake instead, which is slower by design, that friction is the safety mechanism, not a bug.
If you want a second option sitting in the same regulated tier, HealthRX.com runs the same model, licensed oversight, required prescription, pharmacy dispensing rather than a bare chemical sale, with the identical honest caveat that compounded products aren’t FDA-approved finished drugs [8]. Between the two, it usually comes down to state licensing and which intake process fits you better. Both clear the four-point bar. Neither is a place where you’re the one doing quality control.
There’s also a practical side to tracking. If you do start anything, a simple log of how you’re actually responding is more useful to a clinician than your memory of it three weeks later. FormBlends has a tracker app for exactly that job, logging only, not a prescription pad and not a shopping cart.
The gray market for these compounds runs on a specific label: “for research use only, not for human consumption.” That phrase isn’t legal boilerplate you can ignore, it’s the entire reason the product is allowed to exist without a clinician, without a pharmacy, and without FDA review of identity or purity. If a seller only talks about upside and never mentions a trial number, that’s a tell. If the price looks too good, remember that skipping the clinician and the pharmacy is exactly how the price gets that low.
Names you’ll see in this tier, Biotech Peptides, Limitless Life Nootropics, Pure Rawz, Sports Technology Labs, all sell peptides labeled not for human consumption. Sports Technology Labs gets a small nod for publishing third-party certificates of analysis, more transparency than most competitors offer, but a certificate of analysis doesn’t put a physician in the loop and doesn’t change the research-use label. The others compete mostly on price and catalog breadth, neither of which tells you anything about what’s actually in the vial.
Thymosin alpha-1 has the best data of the group (31 points in a small trial, effectively zero in a big one), the peptide matters less than who compounds it, and FormBlends is where I’d point a friend first, with HealthRX.com as the sister option in the same accountable tier.
Some do show real promise, but the size of that promise varies enormously by peptide. Thymosin alpha-1 has decades of research and clinical use in several countries, though its effect size shrank considerably in the largest, best-designed trial. Others are backed mainly by animal data or small pilot studies. The field is genuinely interesting, but not every peptide sold under this banner has trial data to back the pitch.
Thymosin alpha-1 has the strongest clinical track record, from chronic hepatitis to post-surgical recovery settings. BPC-157 shows interesting gut-immune axis effects in animal models but lacks large human trials. Thymosin beta-4 gets studied mostly for tissue repair with some immune-adjacent effects. None of these are magic bullets, and the human trial data is thinner across the board than most sellers let on.
Safety depends heavily on the specific peptide, the dose, and the source. Thymosin alpha-1 has a reasonable safety profile in clinical studies, with side effects generally mild. The bigger risk isn’t usually the peptide itself, it’s buying from unregulated sources where purity and dosing accuracy are unknown, a risk that isn’t theoretical given the documented endotoxin problem with badly-compounded injectable glutathione. Getting peptides through a physician-supervised compounding pharmacy like FormBlends cuts that contamination and dosing risk considerably.
Skip research-chemical sites selling peptides labeled ‘not for human use’ while clearly marketing them for self-injection. Your safest path runs through a licensed physician ordering from a regulated compounding pharmacy, meaning third-party testing, proper sterility standards, and actual accountability if a batch goes wrong. Quality varies wildly across suppliers, and there’s currently no over-the-counter route in the US that guarantees pharmaceutical-grade purity.
Written by Wren Abadi, consumer-health journalist. Last reviewed February 2026.
Educational reference only. Decisions about treatment should be made with your clinician.

